Healthcare Doesn't Have a Pipeline Problem. It Has a Buyer Map Problem
Deconstructing why single-threaded selling is one of the most expensive mistakes in healthcare go-to-market.
There is a gap we consistently see in healthcare GTMs that almost never gets named directly.
A company has a solid pipeline. The CRM looks healthy. A promising deal has been active for six months. The rep has a strong relationship with the VP of Clinical Operations. Leadership feels confident.
Then the deal stalls. A new stakeholder surfaces, procurement gets involved, IT flags a compliance question, and a deal that felt close is back to square one.
The pipeline wasn't wrong. The buyer map was incomplete.
This is one of the most common and most expensive problems in healthcare go-to-market.
The Way Healthcare Actually Buys
Healthcare is not a single-buyer market. It never has been. But the way most commercial teams build their go-to-market motion still treats it like one.
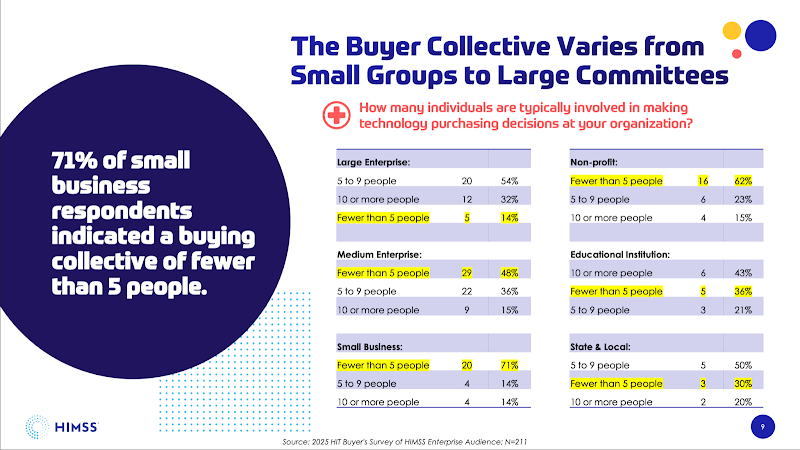
Nearly 60% of organizations report five or more decision-makers in a technology purchase, with 23% reporting ten or more, according to HIMSS's 2025 Healthcare IT Buyer Survey, Major technology decisions involve six to ten stakeholders across clinical, operational, financial, and IT functions. In larger IDNs, that number goes higher.
And critically, the economic buyer and the clinical champion are often different people, operating on different timelines, with different definitions of success.
What this means in practice is that a rep can build a genuinely strong relationship with one person inside a health system and still lose the deal. Not because the champion wasn't sold, but because the champion couldn't sell it internally. And no one on the commercial side mapped the rest of the room.
This isn't purely a healthcare problem, but healthcare makes it worse. The 2026 State of B2B GTM Strategy report, drawing on 511 professionals across the U.S. and U.K., found that nearly 30% of organizations lack alignment around shared GTM goals. In most markets, that's friction. In healthcare, where extended sales cycles and layered decision-making are simply the terrain, it becomes a structural liability.
Why it gets missed in healthcare specifically
Part of this is structural. Access in healthcare is harder than in most markets. Getting time with a CMO or a CFO takes real work. So when a rep finds a champion who is engaged and responsive, there is a natural gravitational pull toward that relationship. It feels like progress. And it is. But it is not sufficient.
The other part is organizational. Our 2026 GTM report also found that roughly 24% of GTM spend goes to initiatives with no traceable commercial outcome. In multi-stakeholder sales, a significant portion of that waste is almost certainly content and campaigns that never reached the full buying committee.
Most marketing teams build content and campaigns for the champion they know. The clinical buyer. The department head. The innovation leader. While the rest of the committee, the people who will ultimately say yes or no in the formal decision process, often see nothing from the vendor until the deal is already in the late stages.
And late stages is the wrong time to introduce yourself to a CFO or a CISO.
By then, you are no longer building trust. You are defending a position.
What a buyer map actually looks like
The organizations getting this right do not wait for the RFP to understand who is in the room. They map it early, and they build the go-to-market motion around the full committee, not just the champion.
In the last issue, we wrote about change management being the hidden revenue killer. The buyer map problem is one of its most common expressions. Here is the framework that closes that gap.
1. Define the committee by account type
For a regional health system, the typical committee looks different than for a large IDN or a specialty group. Build stakeholder maps for each of your core account segments. Name the roles. Define their priorities. Understand their veto points.
2. Create content for each role, not just each stage
Most funnel content is built for awareness, consideration, and decision. That maps to marketing logic, not buyer behavior. And for most teams, the funnel ends at the signature. That is where the relationship with half the buying committee is only getting started. Build content that addresses the specific concerns of each stakeholder. The CFO needs ROI framing. IT needs security and integration evidence. Clinical needs workflow fit and outcomes data.
These are different documents.
And the content doesn't stop at the signature. What you leave a C-suite leader or board member with after the decision is made shapes whether they become an advocate or a skeptic. A one-page outcomes summary sixty days post-implementation. A quarterly value report tied to the metrics they said mattered in the buying process. A clear answer to the question every executive asks internally: was this the right call? That content builds loyalty. It also builds the reference relationships and renewal conversations that most healthcare GTM teams leave entirely to chance.
3. Give your champion the tools to sell internally
Your champion is not just a buyer. In complex deals, they are an internal seller. If they cannot articulate your value to finance, IT, and compliance, you will stall at the point where it matters most. Arm them with the right materials. Make their job easier.
4. Track multi-threaded engagement, not just champion activity
If your CRM only shows contact and activity for one person per account, you are not measuring the deal, you are measuring a relationship. Build your tracking to reflect the full committee. If engagement is single-threaded, that is a signal, not a comfort. And tracking should not stop at the close. If the CFO who approved the deal never hears from you again until renewal, that is a gap in the motion, not just a gap in the relationship.
The 2026 GTM report notes that roughly 21% of companies either lack a formal GTM strategy or have no clear ownership structure. Without that foundation, multi-threaded tracking rarely gets built because nobody has the mandate to do so.
Teams know they need multi-stakeholder coverage. It shows up in strategy decks and QBR conversations. But when you look at how deals are actually worked, the behavior hasn't changed. The tools may have. The language has. The motion hasn't.
That gap between what a team says it does and what it actually does is where revenue leaks.
In a recent episode of Healthcare Marketing Executive I recorded at VIVE with one of our clients Bruce Brandes, Board Chairman at WhaleHawk a healthcare focused ai intelligence platform, he said it best, “The reality is, healthcare decisions are complex and influenced by a range of factors. If you’re not aligning to those dynamics, you’re likely chasing deals that were never going to happen.” Bruce has been in healthcare for over 3 decades with multiple wins under his belt, the most recent being scaling care.ai to Stryker. Listen to the full episode here.
Fixing the buyer map is not a technology problem. And it is not solved by adding another field in the CRM. It requires a deliberate change in three things: how commercial teams think about an account, how marketing builds content, and how leadership measures deal quality beyond the close.
The pipeline number is a lagging indicator. The buyer map is a leading one.
If your deals are stalling in late stages, that is worth diagnosing before you add more pipeline at the top.

Turn Healthcare
Insight
into Accelerated Growth
Our healthcare growth teams works closely with you to design strategies tailored to your unique goals and market dynamics, fully focused on growth.
Accelerating your growth with expert strategies in marketing, branding, research & insights, sales and lead generation to maximize healthcare impact.